AML has one of the lowest survival rates among leukaemias1
Patients who are FLT3 mutation-positive may have a worse prognosis, with higher rates of relapse and lower rates of survival, than patients in the overall AML population2-4
The multiple oncogenic drivers of newly diagnosed acute myeloid leukaemia (AML), including FLT3 mutations, are a central cause of the poor outcomes that define this cancer.5,6
AML survival rates after 5 years1,3,4,7
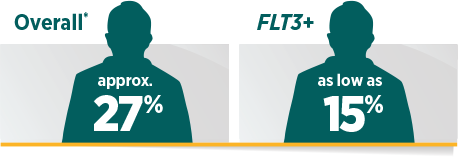
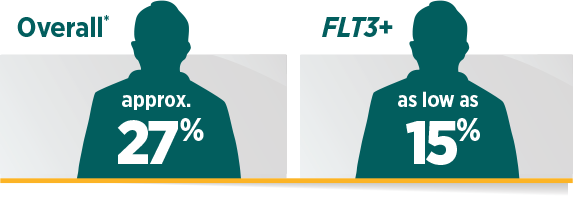
Relative survival based on data of US AML patients from 2007 through 2013.
For decades, there have been few pharmacological advances in AML2,8
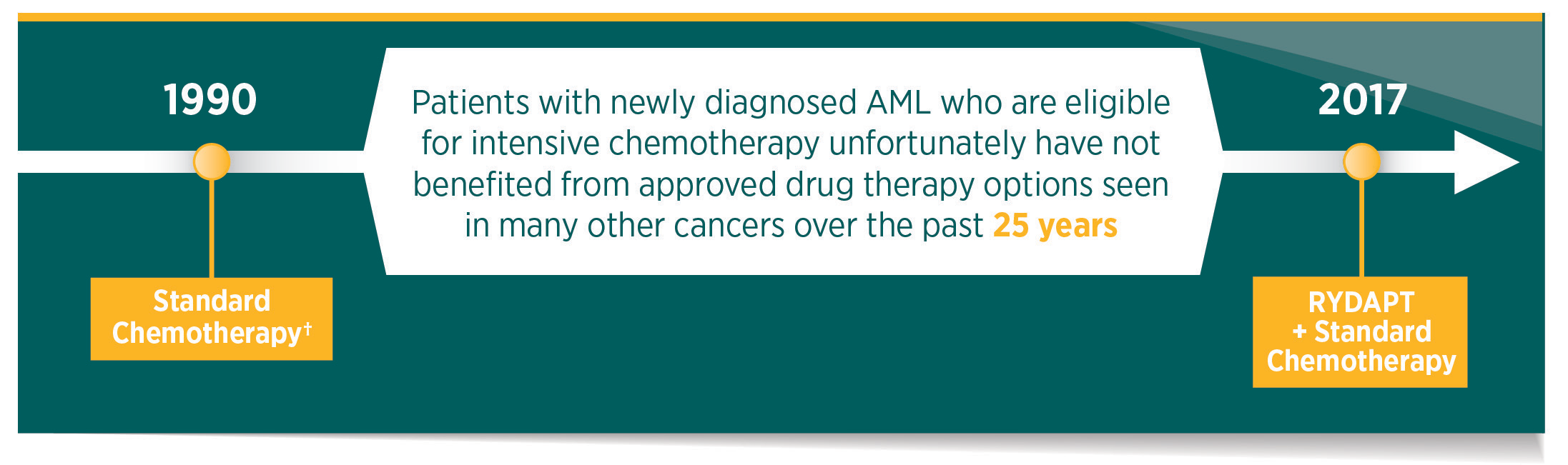
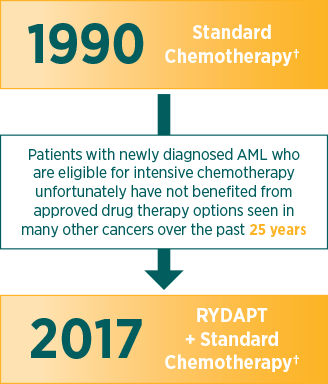
Standard chemotherapy is induction therapy with cytarabine and daunorubicin, and consolidation therapy with high-dose cytarabine.
FLT3, FMS-like tyrosine kinase 3.
References: 1. Howlader N, Noone AM, Krapcho M, et al, eds. SEER Cancer Statistics Review, 1975-2014. Bethesda, MD: National Cancer Institute; 2017. http://seer.cancer.gov/csr/1975_2014/. Updated June 28, 2017. Accessed September 7, 2017. 2. Ferrara F, Schiffer CA. Acute myeloid leukaemia in adults. Lancet. 2013;381(9865):484-495. 3. Gale RE, Green C, Allen C, et al; Medical Research Council Adult Leukaemia Working Party. The impact of FLT3 internal tandem duplication mutant level, number, size, and interaction with NPM1 mutations in a large cohort of young adult patients with acute myeloid leukemia. Blood. 2008;111(5):2776-2784. 4. Mead AJ, Linch DC, Hills RK, Wheatley K, Burnett AK, Gale RE. FLT3 tyrosine kinase domain mutations are biologically distinct from and have a significantly more favorable prognosis than FLT3 internal tandem duplications in patients with acute myeloid leukemia. Blood. 2007;110(4):1262-1270. 5. Levis M. FLT3 mutations in acute myeloid leukemia: what is the best approach in 2013? Hematology Am Soc Hematol Educ Program. 2013;2013:220-226. 6. Döhner H, Weisdorf DJ, Bloomfield CD. Acute myeloid leukemia. N Engl J Med. 2015;373(12):1136-1152. 7. Fathi AT, Chabner BA. FLT3 inhibition as therapy in acute myeloid leukemia: a record of trials and tribulations. Oncologist. 2011;16(8):1162-1174. 8. Lin TL, Levy MY. Acute myeloid leukemia: focus on novel therapeutic strategies. Clin Med Insights Oncol. 2012;6:205-217.